
Region
Lower Extremity

Thigh and Hip
Patients are placed in standardized positions or "views" which were developed to facilitate quick recognition of normal versus abnormal bone structure. In the case of radiographs of the hip, the most frequently used views are:
- Anteroposterior AP hip
- Lateral ("frog-leg")
- AP Pelvis, including upper femora (bilateral)

Radiographs are commonly used to evaluate hip fractures, bone lesions or arthritis. They are also the initial imaging modality of choice for evaluating a patient with hip pain, or evaluating a patient following trauma. Other imaging techniques which may be used for supplemental information include:
CT: can be helpful for complex fractures and dislocations
MRI: hip pain of unknown etiology, infection, tumor, joint space abnormalities and osteonecrosis
Arthrography: evaluates joint anatomy, particularly the acetabular labrum, articular cartilage and ligaments.
AP Hip
For this view, the patient is placed in a supine position with legs together, hips and knees extended, and the feet inverted (turned inwards) 15 degrees. The foot inversion brings the anteverted femoral neck into a plane perpendicular to the radiograph. If properly positioned, the lesser trochanter should be posterior (its tip may project slightly across the medial border of the femur).
Identify the following structures:
- Margin Of Acetabulum
- Hip Joint Space
- Fovea (Capitis)
- Greater Trochanter
- Lesser Trochanter
- Intertrochanteric Crest And Line
Lateral Hip ("frog leg")
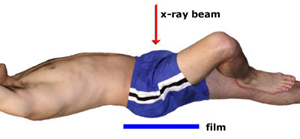
The patient rests in a supine position and externally rotates, flexes, and abducts the femur (the "frog-leg" position, see figure below). As with the AP image, the x-ray beam is directed anterior to posterior across the joint.

This view can be used to evaluate many of the same structures and relations discussed in the AP view. Note in particular that the lesser trochanter is clearly visible (external rotation moves it to a more anterior position) and the greater trochanter is harder to discern (it has been rotated posteriorly). Realize that the angle of the femoral neck cannot be evaluated in this view.
AP Pelvis and Bilateral Upper Femur
This view allows assessment of symmetry of the pelvis and the proximal femurs as they articulate at the hip joint (by comparing the right and left sides).
Identify the following structures:
- Acetabulum
- Fovea
- Pubic Tubercle
- Iliopectineal Line (Pectineal Line)
- Ilioischial Line (This Is A Radiologic Term)
- Femoral Neck
- Greater Trochanter
- Lesser Trochanter
- Ischial Tuberosity
- Obturator Foramen

MRI: Axial Thigh (upper)
This is an axial image of the upper thighs in a male. Fat appears bright in this image, while ligaments, cortical bone and fascia appear dark. Note that the medullary space of the femurs is white, due to the presence of fat in the marrow. Blood vessels appear dark gray or black; this is called a "flow void" and is the normal, expected appearance.
Identify the following structures:
- Anterior Compartment
- Medial Compartment
- Gluteus Maximus
- Scrotum
- Femur
- Sartorius
- Quadriceps Femoris
- Great Saphenous Vein
- Femoral Vessels
- Medial Compartment
- Adductor Longus & Brevis
- Adductor Magnus
- Gracilis
- Hamstring Muscle Group
- Sciatic Nerve

MRI: Axial Thigh (mid)
This is an axial image of the mid thigh of the right lower extremity. The right side of the image is medial, and the left side of the image is lateral. If you recall that all axial images are displayed, by convention, as though you were standing at the foot of the table and looking towards the patient's head, you can reason that this must be the right leg. The same imaging parameters were used as in the prior image.
Identify the following structures:
- Anterior Compartment
- Posterior Compartment
- Medial Compartment

MRI: Axial Thigh (lower)
This is an axial image of the lower thigh of the right lower extremity. The right side of the image is medial, and the left side of the image is lateral. If you recall that all axial images are displayed, by convention, as though you were standing at the foot of the table and looking towards the patient's head, you can reason that this must be the right leg. The same imaging parameters were used as in the prior image.
Identify the following structures:
- Popliteal Artery & Vein
- Sciatic Nerve
- Vastus Lateralis
- Rectus Femoris Tendon
- Vastus Intermedius
- Vastus Medialis
- Sartorius
- Gracilis
- Great Saphenous Vein
- Biceps Femoris (Long & Short Heads)
- Semitendinosus
- Semimembranosus

Thigh and Hip Questions
Radiology Quiz
Quiz

Osteology Quiz
Quiz

Anatomy Quiz
Quiz
Which of the following contributes to the floor of the femoral triangle?
adductor brevis
illiopsoas
gracilis
rectus femoris
sartorius
Knee and Leg
Patients are usually positioned for radiographs according to standard protocols, so that normal patterns can be discerned and abnormalities can be more readily identified. In the case of radiographs of the knee and leg, the most frequently used standard views are:
- Anteroposterior (AP)
- Lateral
- Sunrise (knee)

These may be supplemented by oblique views. It is important to remember that multiple views of a given area may be required in order to determine the actual three-dimensional relationships. Comparison to films of the patient’s other knee can also be useful.
MRI(magnetic resonance imaging) of the knee allows excellent visualization of the internal soft tissues of the knee, including the menisci, articular cartilages, ligaments, tendons, and muscles.
CT (computed tomography) of the knee can be used to further evaluate complex fractures and other abnormalities of bone.
AP Knee
The patient is in a supine position with the knee extended. Three bones comprise the knee joint, the femur, tibia, and patella. Notice that the joint space appears large because the menisci and cartilage are not visible on a plain radiograph. In patients with degenerative joint disease (osteoarthritis), there is often narrowing of the joint space due to the loss of cartilage.
AP Knee, child


The image on the left is an AP view of a child's knee and shows open epiphyseal growth plates. The radiograph on the right is from an adult.
In children, injury to an epiphyseal plate is especially worrisome because the fracture may devascularize the epiphysis and lead to growth disturbances.
In the radiograph of the adult knee, the bones have reached maturity and the epiphyseal plates have ossified. These epiphyseal scars indicate the prior position of the epiphyseal plates.
Lateral Knee
When taking a lateral knee film, flexion of 20 to 30 degrees is usually preferred because this position relaxes the muscles and shows the maximum volume of the joint space.
Identify the following structures:
- Patella
- Fibula
- Borders Of The Femoral Condyles
- Superior Articular Surfaces Of Tibial Condyle

Sunrise View
The sunrise view is a tangential look at the flexed knee. The patient is positioned so that the long axis of the patella is parallel to the x-ray beam, perpendicular to the film cassette/detector. This view is used to assess the patellofemoral articulation, which may be altered by degenerative joint disease.
The femur and tibia are superimposed. Typically the medial femoral condyle is more rounded and/or prominent than the lateral femoral condyle.
Identify the following structures:
- Patella
- Edge Of The Medial Femoral Condyle
- Edge Of The Lateral Femoral Condyle
- Edge Of The Tibia

MRI: Sagittal Knee
The following three MRI images of the knee are T2-weighted images in the sagittal plane, moving from lateral to medial. Fat and fluid appear bright, while ligaments, tendons, and cortical bone appear dark. Since bone marrow contains fat, it appears bright on these T2-weighted images. Muscles are shades of gray.
This image is taken through the lateral aspect of the knee.
Identify the following structures:
- Femur
- Tibia
- Fibula
- Patella
- Patellar Ligament
- Infrapatellar Fat
- Lateral Meniscus
- Gastrocnemius
- Soleus
- Biceps Femoris

MRI: Coronal Left Knee
The next two MRIs show the knee in the coronal plane. This image is roughly in the middle of the knee joint, and the next image is more posterior. View these images as though facing the patient. The left side of the image is medial.
These images are T2-weighted, however the fat signal has been 'suppressed' making structures containing fat appear dark, like the subcutaneous fat and the fatty bone marrow.
Identify the following structures:
- Femoral Condyles
- Tibia
- Medial And Lateral Menisci
- Articular Cartilage
- Synovial Fluid
- Anterior Cruciate Ligament
- Posterior Cruciate Ligament
- Medial Collateral Ligament

MRI: Axial leg
This is an MRI of the mid-left leg. Note that tendons and cortical bone appear dark in this image, while subcutaneous fat & fat in the marrow spaces appears bright.
Identify the following structures:
- Posterior Compartment
- Anterior Compartment
- Lateral Compartment

Dissection of the Knee
Knee and Leg Questions
Radiology Quiz
Quiz

Osteology Quiz
Quiz

Anatomy Quiz
Quiz
Which ligament prevents medial displacement of the tibia with respect to the femur?
anterior cruciate
fibular collateral
posterior cruciate
tibial collateral
Foot and Ankle
The standard views for foot and ankle include:
- AP radiograph of the ankle
- Lateral Ankle
- AP and Oblique Foot
Identify the following structures:
- Tibia/medial Malleolus
- Fibula/lateral Malleolus
- Talus
- Cuboid
- Metatarsals

Lateral Foot
On a lateral radiograph of the foot, most of the mid-foot and fore-foot bones overlap and are difficult to identify individually. This view is useful to demonstrate the neck of the talus and the anterior portion of the calcaneus.
Identify the following structures:
- Talus
- Calcaneus
- Navicular
- Cuboid
- Cuneiform Bones
- Metatarsal Bones
- Sesamoid Bones

Dissection of the Foot
Foot and Ankle Questions
Radiology Quiz
Quiz

Osteology Quiz
Quiz

Nerves of the Lower Extremity
Femoral Nerve
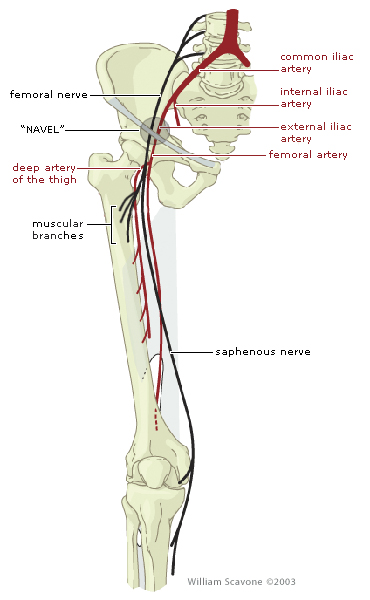
The femoral nerve is formed by the ventral rami of L2-L4, specifically the posterior divisions of the lumbar plexus.
The femoral nerve travels posterior to the inguinal ligament within the muscular lacuna. The muscular lacuna also contains the iliopsoas muscle.
NAVEL is a mnemonic for remembering the neurovascular structures that travel deep to the inguinal ligament into the femoral triangle.
N = femoral nerve A = femoral artery V = femoral vein EL = empty space (femoral canal) and lymphatics
The femoral nerve provides motor innervation to the muscles of the anterior compartment of the thigh, with a few exceptions: -the psoas portion of iliopsoas is innervated by muscular branches of the lumbar plexus -tensor fasciae latae is innervated by the superior gluteal nerve -pectineus is occasionally innervated by the obturator nerve
The femoral nerve provides sensory innervation to the skin of the anterior thigh and the anteromedial aspect of the leg. The afferent innervation of the leg is provided by the saphenous nerve (a branch of the femoral nerve that travels in the adductor canal).
Injury to the femoral nerve typically produces: weakness of hip flexion, loss of knee extension (no patellar reflex), and sensory loss over the territories described above.
Sciatic Nerve

The sciatic nerve is formed by the ventral rami of L4-S3.
The sciatic nerve is comprised of the tibial nerve and common fibular nerve surrounded by a common epineurium.
The sciatic nerve exits the pelvis via the greater sciatic foramen, typically inferior to piriformis muscle.
The sciatic nerve provides motor innervation to the muscles of the posterior compartment of the thigh, the "hamstring portion" of adductor magnus and all muscles of the leg and foot.
The sciatic nerve provides sensory innervation to the skin of the lateral aspect of the leg (anterolateral and posterolateral), and almost all of the foot (exception is the medial part of the foot that is innervated by saphenous nerve).
Injury to the sciatic nerve typically produces: complete motor loss of the muscles of the posterior thigh, leg and foot; sensory loss over the territories described above.
Tibial Nerve

The tibial nerve is a component of the sciatic nerve. It is formed from the anterior divisions of the sacral plexus.
The tibial nerve travels in the posterior leg with the posterior tibial artery, in the fascial plane between the superficial and deep muscle groups. It passes posterior to the medial malleolus at the ankle ("Tom, Dick and very nervous Harry").
"Tom, Dick and very nervous Harry" is a mnemonic for remembering the structures that pass posterior to the medial malleolus at the ankle.
T = tibialis posterior tendon D = flexor digitorum tendon A = posterior tibial artery V = posterior tibial veins (usually a pair on either side of the artery) N = tibial nerve H = flexor hallucis longus tendon
The tibial nerve provides motor innervation to the muscles of the posterior compartment of the leg (both superficial and deep).
The tibial nerve provides sensory innervation to the posterior aspect of the leg (via its contribution to the sural nerve) and the sole of the foot.
The tibial nerve terminates by bifurcating into the medial and lateral plantar nerves in the sole of the foot.
Injury to the tibial nerve typically produces: loss of plantarflexion of the foot, loss of flexion of the toes and weakened inversion of the foot; sensory loss over the territories described above.
Common Fibular Nerve

The common fibular nerve is a component of the sciatic nerve. It is formed from the posterior divisions of the sacral plexus. In the past, common fibular nerve was called "common peroneal nerve".
The common fibular nerve travels around the neck of the fibula in a superficial position - here it is vulnerable to injury.
Near the neck of the fibula, the common fibular nerve divides into superficial and deep branches. Its motor and sensory innervation will be described in the context of these branches on the next two pages.
Superficial Fibular Nerve
The superficial fibular nerve arises from the common fibular nerve near the neck of the fibula.
The superficial fibular nerve travels in the lateral compartment of the leg.
The superficial fibular nerve provides motor innervation to the muscles of the lateral compartment of the leg (muscles that evert the foot).
The superficial fibular nerve provides sensory innervation to the anterolateral aspect of the leg (the distal half) and the dorsum of the foot (the exception is the webspace between the hallux and second digit).
Injury to the superficial fibular nerve typically produces loss of eversion of the foot, and sensory loss over the territories described above.
Deep Fibular Nerve
The deep fibular nerve arises from the common fibular nerve near the neck of the fibula.
The deep fibular nerve travels in the anterior compartment of the leg on the anterior surface of the interosseous membrane (it travels with the anterior tibial artery).
The deep fibular nerve provides motor innervation to the muscles of the anterior compartment of the leg (muscles that primarily dorsiflex the foot and extend the toes).
The deep fibular nerve provides sensory innervation to the webspace between the hallux and second digit.
Injury to the deep fibular nerve typically produces loss of dorsiflexion of the foot, loss of extension of the toes, and sensory loss in the first webspace.
Foot Drop

Because of its superficial position, the common fibular (peroneal) nerve is the most frequently injured nerve in the lower limb.
As the common fibular (peroneal) nerve leaves the popliteal fossa, it descends on the posterior aspect of the head of the fibula. It then winds around the fibular neck (arrow) where it is susceptible to trauma, such as a blow to the lateral aspect of the leg or fracture of the neck of the fibula.
Severance of the common fibular (peroneal) nerve results in paralysis of all muscles in the anterior and lateral compartments of the leg. This loss of dorsiflexion of the ankle and eversion of the foot causes foot-drop. Because the patient is unable to make the heel strike the ground first, he will have a high stepping gait in which the affected foot is raised higher than normal so that the toes do not hit the ground. In addition, the foot is brought down suddenly, producing a “clopping” sound.
Vasculature and Angiography
Left Lower Extremity Angiogram
The video below shows a series of images from a lower extremity angiogram. A catheter was placed via the left common femoral artery with the tip positioned in the left external iliac artery. Contrast is being injected through the catheter as sequential images are obtained to follow the contrast as it travels down the arteries of the leg.
Observe the following:
The multiple branches originating from the profunda femoral artery, supplying the thigh musculature. Note the relative paucity of branches originating from the superficial femoral artery.
The relatively straight course of the popliteal artery, and its bifurcation into the anterior tibial artery, more lateral, and the tibioperoneal trunk, more medial.
The posterior tibial artery is dominant in this patient; larger in caliber than the anterior tibial, and contributing more blood flow to the foot.
Bilateral Lower Extremity Angiogram: SFA Occlusion
Contrast is being injected through a catheter that was inserted via the left common femoral artery. The catheter tip is in the distal aorta. Sequential images are obtained at multiple "stations" to follow the contrast as it travels down the arteries of the legs. The bones have been subtracted from the image.
Observe the following:
The injected contrast material mixes with the blood, opacifying it. It is propulsed antegrade down the arteries of the legs via cardiac output. As unopacified blood flows into the lower extremity, it "washes out" the high density contrast.
Blood flow in the right superficial femoral artery is slightly slower than in the left, due to a focal SFA occlusion. Branches of the right profunda femoral artery reconstitute the SFA distal to the stenosis. Note that the wash out of opacified blood is slower in the right leg than the left, due to slower flow.
There is also a focal stenosis of the right SFA/popliteal artery junction.
Femoral Artery
The femoral artery is a continuation of the external iliac artery (name changes as it passes deep to the inguinal ligament).
The femoral artery is found at the midpoint of the inguinal ligament. The femoral pulse is palpable at this midinguinal point.
NAVEL is a mnemonic for remembering the neurovascular structures that travel deep to the inguinal ligament into the femoral triangle.
N = femoral nerve A = femoral artery V = femoral vein EL = empty space (femoral canal) and lymphatics
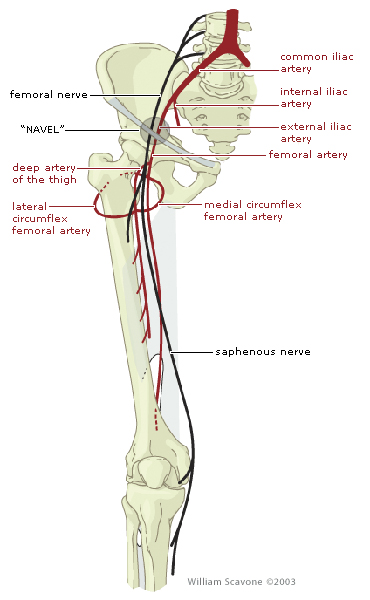
The deep femoral artery arises in the femoral triangle. It passes deep to the adductor longus and gives rise to perforating arteries that supply the posterior thigh.
The medial and lateral femoral circumflex arteries are typically branches of the deep femoral artery. The medial branch is particularly important as it is the major blood supply to the head and neck of the
Femoral Angiogram
A catheter was placed into the left common femoral artery. Contrast injected through the catheter opacifies the left thigh vasculature. The image on the left is a digital subtraction image; the bones have been subtracted out. This results in greater conspicuity of the vascular structures.
The bony structures can be identified and used as landmarks. Names of arteries often change after they pass a certain anatomic landmark, such as the external iliac artery becoming the femoral artery distal to the inguinal ligament.
Identify the following structures:
- Common Femoral Artery
- Superficial Femoral Artery
- Deep Femoral Artery
- Catheter

Popliteal Artery

The popliteal artery is a continuation of the femoral artery (name changes as femoral travels through the adductor hiatus).
The popliteal pulse is palpable in the popliteal fossa (pulsations are best felt in the inferior part of the fossa with the knee flexed and relaxed).
Genicular branches arise posterior to the knee joint and contribute to the collateral circulation around the knee joint.
The popliteal artery terminates by bifurcating into the anterior and posterior tibial arteries.
Anterior Tibial Artery

After arising from the popliteal artery, the anterior tibial artery travels into the anterior compartment of the leg by passing between the tibia and fibula through a gap in the interosseous membrane.
Anterior tibial artery travels inferiorly on the anterior surface of the interosseous membrane with the deep fibular nerve.
Anterior tibial artery primarily provides blood to the muscles of the anterior compartment of the leg. It also contributes to the collateral circulation of the knee and ankle, via its recurrent branch and anterior malleolar branches, respectively.
Anterior tibial artery changes its name to dorsalis pedis artery when it crosses the ankle joint.
Posterior Tibial Artery

After arising from the popliteal artery, the posterior tibial artery travels in the medial part of the posterior compartment of the leg in the fascial plane between the superficial and deep muscle groups.
At its proximal end, the posterior tibial artery gives off the fibular artery, which travels in the lateral part of the posterior compartment of the leg. The fibular artery has perforating branches that pierce the intermuscular septum to enter the lateral compartment of the leg.
The posterior tibial artery provides blood to the muscles of the posterior and lateral compartments of the leg and the sole of the foot. It also contributes to the collateral circulation of the ankle joint.
The posterior tibial artery is found posterior to the medial malleolus at the ankle in association with the same named veins and tibial nerve. The posterior tibial pulse can be palpated in this location.
"Tom, Dick and very nervous Harry" is a mnemonic for remembering the structures that pass posterior to the medial malleolus at the ankle.
Popliteal Angiogram
This image demonstrates the popliteal artery and its relationship to the bony landmarks of the knee. The image on the left is a digital subtraction angiogram. Note how this increases the conspicuity of the smaller arterial branches.
Identify the following structures:
- Popliteal Artery
- Anterior Tibial Artery
- Posterior Tibial Artery
- Peroneal Artery

Infrapopliteal Angiogram
These are three sequential angiographic images of the left lower leg; the image on the left is the most proximal, and on the right the most distal. Bones have been subtracted from the images. The non-subtracted image is shown on the right.

Dorsalis Pedis Artery

The dorsalis pedis artery is a continuation of the anterior tibial artery (name changes when anterior tibial crosses the ankle joint).
The dorsalis pedis artery gives off two tarsal branches (medial and lateral) as it travels superior to the tarsal bones (not labeled on the diagram).
The pulse of dorsalis pedis can be felt by compressing the artery against the tarsal bones - specifically between the tendons of extensor hallucis longus and extensor digitorum longus.
Near the tarsometatarsal joint, the dorsalis pedis artery gives rise to the arcuate artery that can be compared to the dorsal carpal arch of the hand. The arcuate artery has three dorsal metatarsal arteries, which divide into dorsal digital arteries.
The dorsalis pedis artery gives rise to the first dorsal metatarsal artery directly; it then travels deep into the sole of the foot as the deep plantar artery.


